If you have been dealing with stiff, swollen, or painful joints in the morning, you are probably already searching for answers about rheumatoid arthritis symptoms, how the disease progresses, and what you can actually do about it. Rheumatoid arthritis (RA) is one of the most common autoimmune conditions in the world, affecting roughly 1 percent of the global population. Women are two to three times more likely to develop it than men. Understanding how it progresses can genuinely change the outcome of your treatment. The earlier you catch it, the better your chances of protecting your joints for life. This guide breaks down all 4 stages of rheumatoid arthritis, what symptoms to expect at each stage, how rheumatoid arthritis is diagnosed, the best treatment for rheumatoid arthritis available today, and practical advice for living well with RA.
Rheumatoid arthritis is an autoimmune disease. That means your immune system, which normally protects you from infections, mistakenly attacks the lining of your own joints. This lining is called the synovium. When it gets inflamed repeatedly, it thickens and starts damaging the cartilage and bone underneath.
Unlike regular wear-and-tear arthritis (osteoarthritis), RA can affect people in their 30s and 40s, and in some cases even younger. It also does not just stop at the joints. Untreated RA can cause fatigue, persistent fever, and complications in organs like the heart, lungs, and eyes.
RA usually affects joints on both sides of the body at the same time, like both wrists, both knees, or both hands. That symmetrical pattern is one of the key things rheumatologists look for during diagnosis. It can also come in waves, with periods of flare-ups followed by stretches of relative calm called remissions.
Who is at risk?
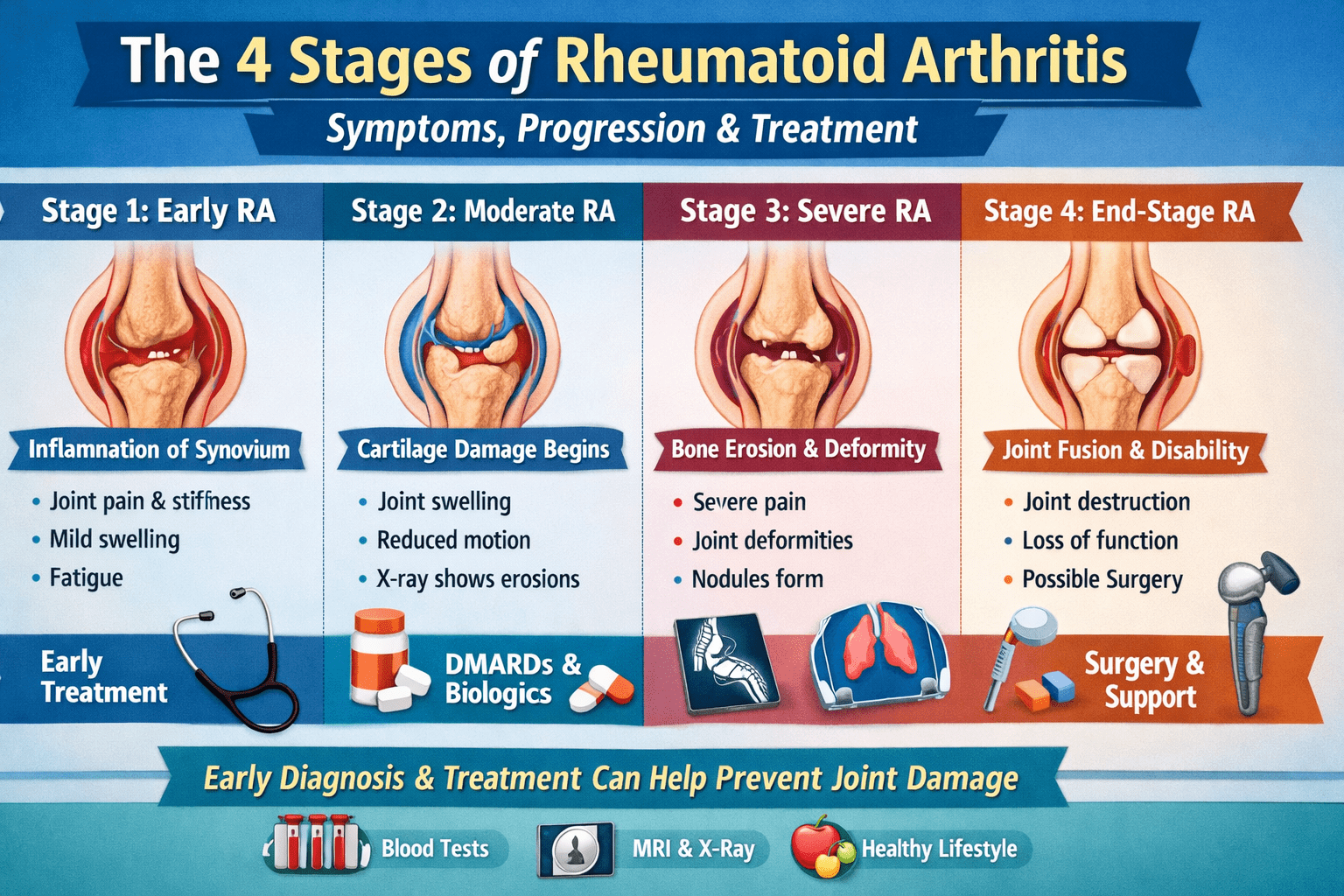
Why Knowing the Stages of Rheumatoid Arthritis Matters
A lot of patients come in after months or even years of dismissing the early signs, assuming it was just tiredness or minor joint pain from overuse. By the time they finally get a rheumatoid arthritis test done, the damage is already at a more advanced stage and some of it cannot be reversed.
The stages of rheumatoid arthritis help doctors understand how far the disease has progressed, what kind of treatment to start, and how aggressively to manage it. Knowing which stage you are in gives both you and your doctor a clearer picture of what is happening inside your joints and what the realistic treatment goals are.
Doctors use a combination of clinical assessment, blood tests, and imaging to determine the stage. The classification system most commonly used today is based on the American College of Rheumatology and European League Against Rheumatism (ACR/EULAR) criteria.
This is when inflammation begins inside the joint lining. At this point, no bone or cartilage has been destroyed yet, but the synovium is already swelling up and becoming irritated.
What happens inside the body at Stage 1:
The immune cells (mainly T cells and B cells) begin gathering in the synovial lining. The tissue starts to thicken. Inflammatory chemicals called cytokines, including TNF-alpha, interleukin-1, and interleukin-6, are already active and driving the process. Even though the damage has not yet reached the bone, this internal chemical storm is already underway.
Symptoms at Stage 1:
Many patients at this stage brush off the symptoms as stress or overwork. The swelling might not even be visible from the outside in early weeks. But if you press on those joints, they feel tender and slightly puffy.
What imaging shows at Stage 1:
Standard X-rays often look completely normal at this stage. However, MRI and musculoskeletal ultrasound are more sensitive and can detect early synovial inflammation, increased blood flow in the joint lining, and very subtle bone changes before they become obvious on X-ray. This is why ultrasound has become an important tool in early RA diagnosis.
Why early detection matters most here:
Stage 1 is genuinely the best window to start rheumatoid arthritis treatment. At this point, medications can suppress the immune response and prevent structural damage from happening at all. Many people who are diagnosed and treated aggressively at Stage 1 go into remission and stay there with careful management. Some achieve what is called a “treat-to-target” outcome, meaning the disease activity drops to minimal or zero and stays there.
By Stage 2, the inflammation has been going on long enough to start affecting the cartilage inside the joint. Cartilage acts as the cushion between bones. When it starts to thin or erode, movement becomes more painful and the joint loses some of its range of motion.
What happens inside the body at Stage 2:
The synovium has now formed what is called a pannus, an aggressive layer of inflamed tissue that grows into the cartilage and begins eating away at it. This pannus releases enzymes that degrade cartilage. The bone beneath the cartilage can start to show tiny erosions at the edges of the joint, called marginal erosions, which are visible on X-ray.
Symptoms at Stage 2:
What imaging shows at Stage 2:
X-rays now begin to show joint space narrowing, which indicates cartilage thinning. Early bone erosions may also be visible at the joint margins. MRI provides a more detailed picture and can quantify the amount of active inflammation (synovitis) alongside structural damage.
Blood markers at Stage 2:
Inflammatory markers like ESR (erythrocyte sedimentation rate) and CRP (C-reactive protein) are usually elevated. Rheumatoid factor and anti-CCP antibodies may already have been positive since Stage 1, but are now almost consistently detected. Doctors use a scoring system called the DAS28 (Disease Activity Score) to measure how active the disease is at this point.
Note for patients in Maharashtra: Many patients reach Stage 2 before they see a specialist. If you are experiencing these symptoms and looking for an arthritis specialist near me in Mumbai or surrounding areas, Stage 2 is still a very treatable point. Rheumatoid arthritis treatment in Mumbai at this stage typically involves starting or intensifying DMARDs, with good results for most patients.
Stage 3 is where the damage becomes more visible and more serious. The cartilage is significantly worn down, and the bones themselves start eroding at the joint surfaces. This is also when joint deformity can begin.
What happens inside the body at Stage 3:
The pannus tissue has now invaded both the cartilage and the underlying bone. Large areas of bone erosion are visible on imaging. The joint may begin to lose its normal alignment, which leads to visible deformity. The tendons and ligaments around the joint can also be affected, further contributing to instability and deformity.
Symptoms at Stage 3:
Common deformities seen at Stage 3:
RA beyond the joints at Stage 3:
This is the stage where extra-articular (outside the joints) complications become more common. These include:
Treatment at Stage 3 often involves a rheumatologist working alongside cardiologists, pulmonologists, and ophthalmologists to manage the full scope of the disease.
At Stage 4, the active inflammation may actually reduce in some patients. But this does not mean things are improving. It often means the joint has been so severely damaged that there is little cartilage or functional tissue left to inflame.
What happens at Stage 4:
The joint space is almost completely gone. In some joints, the bones may fuse together entirely in a process called ankylosis. This results in a joint that has no movement at all. The muscles, tendons, and ligaments around the joint are severely weakened or altered. Pain at this stage is often due to bone-on-bone contact and secondary osteoarthritis rather than active inflammation.
Symptoms at Stage 4:
Treatment at Stage 4:
The focus shifts to pain management, preserving remaining function, and improving quality of life. Surgical options become more relevant at this stage:
Many patients ask how rheumatoid arthritis is diagnosed and why it sometimes takes months to get a confirmed answer. The truth is, RA diagnosis is not based on one single test. It is a combination of clinical findings, blood results, and imaging.
Clinical evaluation:
Your rheumatologist will examine which joints are swollen or tender, how long morning stiffness lasts, whether the inflammation is symmetrical, and what your overall health picture looks like. They will also ask about family history of autoimmune conditions.
Rheumatoid arthritis tests commonly used:
Imaging used in RA diagnosis and monitoring:
The ACR/EULAR 2010 Classification Criteria:
Doctors use a scoring system to classify RA. Points are given based on number of joints involved, type of serological tests (RF, anti-CCP), duration of symptoms (less than or more than 6 weeks), and whether inflammatory markers are elevated. A score of 6 or more out of 10 confirms RA diagnosis.
There is no cure for RA yet. But treatment today is far more effective than it was even 20 years ago. Most people with RA can manage their symptoms well and prevent serious joint damage with the right plan started early enough.
Modern rheumatology follows a “treat-to-target” strategy. This means setting a clear goal (usually remission or at least low disease activity) and adjusting medications every 4 to 8 weeks until that goal is achieved. This approach has significantly improved outcomes compared to older wait-and-see methods.
These are the foundation of RA treatment. They do not just control symptoms. They actually slow or stop disease progression.
Biologics are a newer class of medications that target specific proteins in the inflammatory process rather than suppressing the entire immune system.
Biologics are generally prescribed when conventional DMARDs alone are not controlling the disease adequately. They are given either as injections or infusions.
A more recent oral class of medications that block the JAK-STAT signaling pathway inside immune cells. Examples include:
These are taken as daily pills, which many patients find easier than injections. They are generally used when biologics have not worked well enough or are not suitable.
NSAIDs (like ibuprofen or naproxen) and corticosteroids (like prednisolone) do not slow disease progression. But they are effective at reducing pain and inflammation during flare-ups. Corticosteroids are usually used short-term because long-term use carries side effects like bone loss, weight gain, and blood sugar changes.
These are consistently underutilized in RA management. A physiotherapist can design exercises that maintain muscle strength around affected joints without worsening inflammation. An occupational therapist can suggest adaptive tools and techniques for daily tasks that protect damaged joints. Both have strong evidence behind them for improving quality of life in RA patients.
There is no single “RA diet,” but certain dietary patterns help reduce systemic inflammation. A Mediterranean-style diet, rich in vegetables, oily fish, legumes, and olive oil, is supported by evidence for reducing inflammatory markers. Foods to moderate include processed meats, refined sugar, and excess alcohol. Omega-3 fatty acids (from fish oil) have shown modest anti-inflammatory effects in clinical studies.
Vitamin D deficiency is very common in RA patients and is associated with higher disease activity. Getting vitamin D levels checked and supplementing if needed is a simple step that can support overall immune regulation.
Getting diagnosed and starting treatment is only the beginning. RA requires ongoing monitoring to check whether the treatment is working, catch any side effects early, and adjust the plan as needed.
What monitoring typically involves:
Do not wait until the pain becomes unbearable. Book an appointment if:
If you are based in Maharashtra and searching for an arthritis specialist near me, early consultation with a rheumatologist is the single most important step you can take. Rheumatoid arthritis treatment in Mumbai is now accessible across multiple hospitals and clinics, with specialists trained in the latest biological and targeted therapies. Getting in front of a rheumatologist within the first few weeks of symptoms can be the difference between full remission and long-term joint damage.
Rheumatoid Arthritis vs. Other Types of Arthritis
Patients often confuse RA with other forms of arthritis. Here is a quick comparison:
Rheumatoid Arthritis vs. Osteoarthritis: RA is autoimmune and affects younger people. Osteoarthritis is degenerative and mostly affects people over 50. RA causes symmetrical joint involvement; osteoarthritis tends to affect joints unevenly. RA involves significant systemic symptoms like fatigue and fever; osteoarthritis is mostly localized.
Rheumatoid Arthritis vs. Psoriatic Arthritis: Both are autoimmune. Psoriatic arthritis (PsA) is associated with the skin condition psoriasis. PsA can cause asymmetric joint involvement and a sausage-like swelling of entire fingers or toes (dactylitis). Blood tests for RF and anti-CCP are usually negative in PsA.
Rheumatoid Arthritis vs. Lupus (SLE): Both are autoimmune and can cause joint pain and fatigue. Lupus involves a different set of antibodies (ANA, anti-dsDNA) and a wider range of organ involvement including kidneys and skin. Joint damage in lupus is generally less severe than in RA.
Living With Rheumatoid Arthritis: Practical Advice
A diagnosis of RA is serious, but it is not a life sentence. Thousands of people manage RA well enough to work full-time, exercise regularly, travel, and lead active lives. The key is consistency with treatment and being honest with your doctor about what is and is not working.
Flares are temporary worsening of symptoms. Triggers include stress, infections, skipping medication doses, overexertion, and sometimes no obvious cause at all. Having a clear plan for flares, such as knowing when to use a short course of steroids, when to rest versus when to keep moving, and when to call your doctor, makes them much easier to manage.
Depression and anxiety are significantly more common in people with RA than in the general population. Chronic pain is exhausting, and dealing with a disease that fluctuates unpredictably takes a real psychological toll. Do not ignore this. Many rheumatology centers now have integrated mental health support. Addressing mental health is not separate from managing RA. It is part of it.
RA often improves during pregnancy, particularly in the second and third trimesters. However, it frequently flares after delivery. Some RA medications need to be stopped before or during pregnancy. If you are planning a pregnancy, discuss this with your rheumatologist well in advance so your medications can be reviewed and adjusted safely.
Many people with RA continue working throughout their lives, especially if the disease is well controlled. For those with physical jobs or jobs requiring fine motor skills, early occupational therapy advice and workplace adjustments can help significantly. In India, awareness of workplace accommodations for chronic illness is still limited, but it is worth advocating for.
Understanding the 4 stages of rheumatoid arthritis is not just academic. It gives you the context to act early, ask the right questions, and make informed decisions about your care. Stage 1 and Stage 2 are the windows where treatment does the most good and where joint damage can genuinely be prevented. Stage 3 and Stage 4 are harder, but still manageable with the right medical team.
If you or someone you know has been experiencing morning joint stiffness, symmetrical joint swelling, or unusual fatigue for more than a few weeks, do not dismiss it. Get a proper rheumatoid arthritis test done, see a specialist, and start addressing it with the right support. Rheumatoid arthritis treatment today is better than it has ever been. The earlier you start, the more of your joint health you can protect.